Updated October 2025
The State of Antibody-Drug Conjugate Clinical Trials in 2025
Antibody–drug conjugates (ADCs) are a rapidly expanding class of targeted cancer therapies that combine the specificity of monoclonal antibodies with the potency of cytotoxic agents. These constructs are designed to deliver chemotherapy directly to tumor cells while minimizing damage to healthy tissue. As of 2024, more than 100 ADCs are in clinical development, with 20 FDA-approved indications across hematologic and solid tumors.1
The clinical trial landscape for ADCs is evolving quickly. Sponsors are exploring new payload mechanisms, including topoisomerase inhibitors, DNA alkylators, and microtubule disruptors. Trials are also investigating novel linkers and conjugation technologies to improve stability, reduce off-target toxicity, and enhance tumor penetration. HER2, TROP2, and BCMA remain dominant targets, but newer ADCs are being designed for HER3, CEACAM5, and Nectin-4, expanding the therapeutic reach.1
Dual-payload ADCs are entering early-phase trials, aiming to overcome resistance and tumor heterogeneity by delivering multiple cytotoxins simultaneously. These designs require careful dose optimization and safety monitoring, especially in solid tumors where antigen expression can vary widely. Biomarker-driven enrollment and adaptive trial designs are helping sponsors manage complexity and improve response rates.2
Geographically, ADC trials are concentrated in North America, Europe, and East Asia, with increasing interest in decentralized models to improve access. The regulatory environment is also adapting, with agencies offering expedited pathways for ADCs that demonstrate strong early efficacy and manageable safety profiles.
This article reviews the current ADC trial landscape, including trial status, geographic distribution, patient segments, and therapeutic focus. It also outlines how Precision for Medicine supports sponsors in executing ADC trials with technical precision and operational discipline.

Where ADC Trials Stand Today: A Pipeline Overview
The ADC trial pipeline spans all phases of development indicating sustained investment in clinical validation. Sponsors are balancing risk with opportunity in a competitive space.
ADC Trials by Development Status
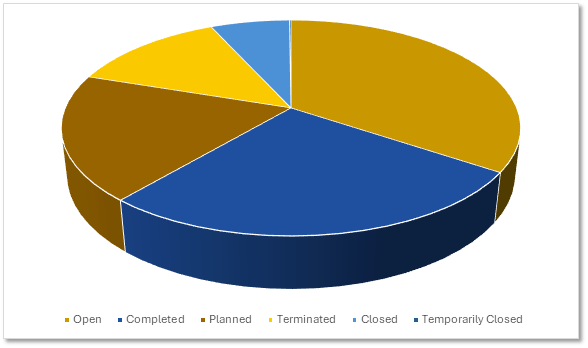 Citeline Trialtrove® – 07OCT2025
Citeline Trialtrove® – 07OCT2025
ADC Trial Activity: Five-Year Growth Trajectory
ADC trial starts have accelerated in recent years mirroring broader oncology trends in targeted therapeutics.
 Citeline Trialtrove® – 07OCT2025
Citeline Trialtrove® – 07OCT2025
Global Footprint: Where ADC Trials Are Happening
ADC trials are geographically concentrated in China and the U.S., followed by Europe, Australia and East Asia.
Planned & Ongoing ADC Trials by Site Country
|
Countries |
Count |
|
China |
812 |
|
United States |
524 |
|
Spain |
233 |
|
Australia |
201 |
|
South Korea |
197 |
|
France |
196 |
|
Italy |
176 |
|
Japan |
175 |
|
United Kingdom |
168 |
|
Canada |
167 |
Citeline Trialtrove® – 07OCT2025
Therapeutic Focus: Cancer Types Leading ADC Development
Therapeutic area trends show a clear emphasis on cancer indications where targeted delivery offers clear advantages. This focus aligns with ADCs' mechanism of action and clinical promise.
Planned & Ongoing ADC Trials by Therapeutic Area
 Citeline Trialtrove® – 07OCT2025
Citeline Trialtrove® – 07OCT2025
Top Cancer Indications in ADC Clinical Research
ADC trials are most common in breast, lung, and esophageal cancers.
Planned & Ongoing ADC Trials by Indication
|
Indication |
Count |
|
Unspecified Solid Tumor |
515 |
|
Breast |
339 |
|
Lung, Non-Small Cell |
327 |
|
Esophageal |
231 |
|
Gastric |
221 |
|
Ovarian |
180 |
|
Colorectal |
140 |
|
Bladder |
139 |
|
Head/Neck |
135 |
|
Pancreas |
121 |
Citeline Trialtrove® – 07OCT2025
Early-Stage Development Dominates ADC Trial Activity
Phase data shows a strong emphasis on early development highlighting the exploratory nature of ADC research. Late-phase trials may increase as early data matures.
Precision for Medicine's ADC Trials by Phase
 Citeline Trialtrove® – 07OCT2025
Citeline Trialtrove® – 07OCT2025
How Precision Drives ADC Clinical Research
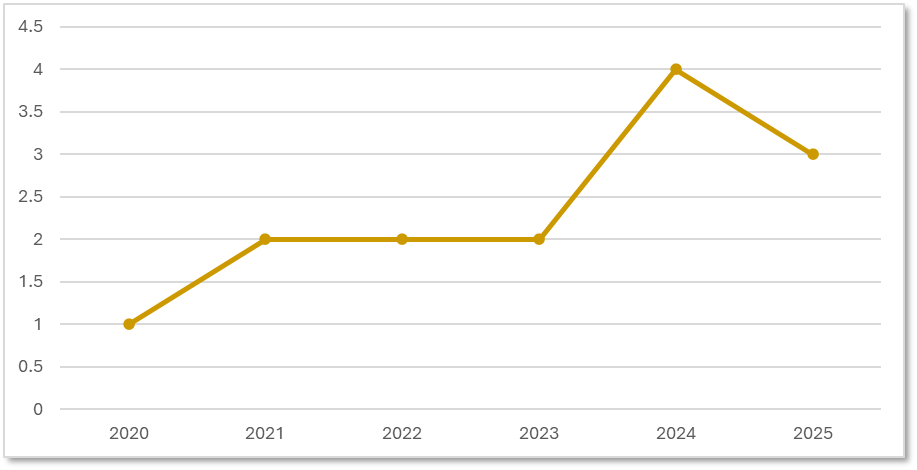
Our ADC Trial Portfolio: Growing with the Market
Precision for Medicine has initiated multiple ADC trials, focusing on the last 5 years we have seen an upward trend, which aligns with overall global trends in targeted oncology. Due to our diverse experience, our study teams are equipped to manage complex ADC protocols, spanning multiple indications.
Precision for Medicine's ADC Trials by Start Date
 Citeline Trialtrove® – 07OCT2025
Citeline Trialtrove® – 07OCT2025
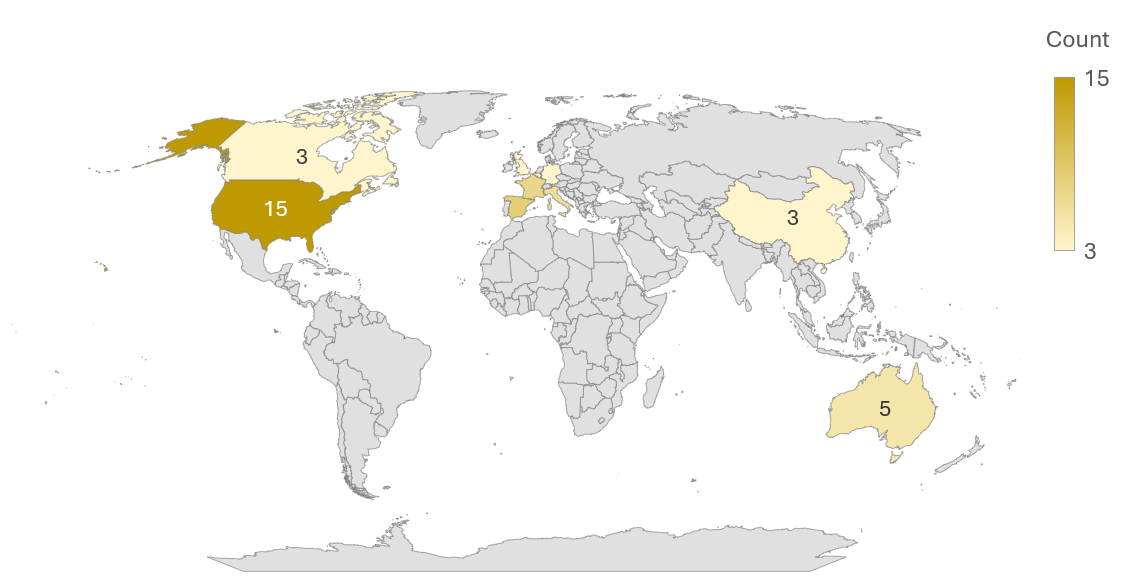
Global Capabilities: Precision's ADC Trial Network
Our geographic footprint includes North America, Europe, and Asia. When it comes to ADC trial execution, Precision adapts to regional nuances.
Precision for Medicine's ADC Trials by Site Country
Citeline Trialtrove® – 07OCT2025
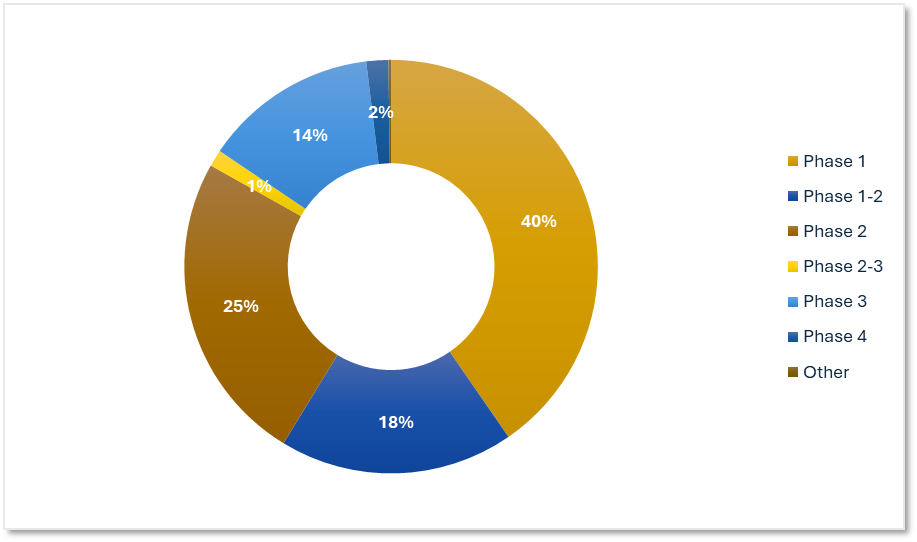
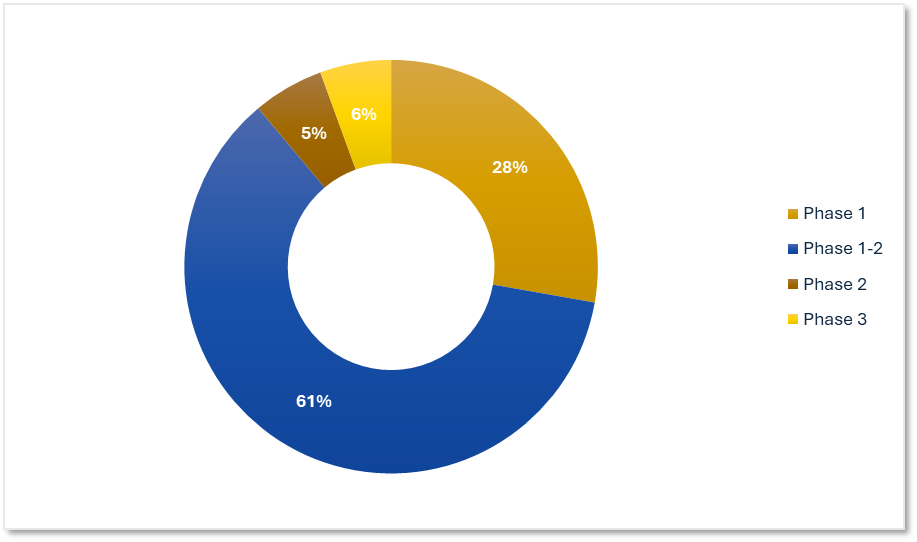
Precision's ADC Trial Experience by Phase
Our work spans early discovery through late-stage validation with a strong presence in Phase 1 and Phase 1-2. Our teams successfully manage dose escalation, biomarker integration, and close safety oversight.
Precision for Medicine's ADC Trials by Phase
 Citeline Trialtrove® – 07OCT2025
Citeline Trialtrove® – 07OCT2025
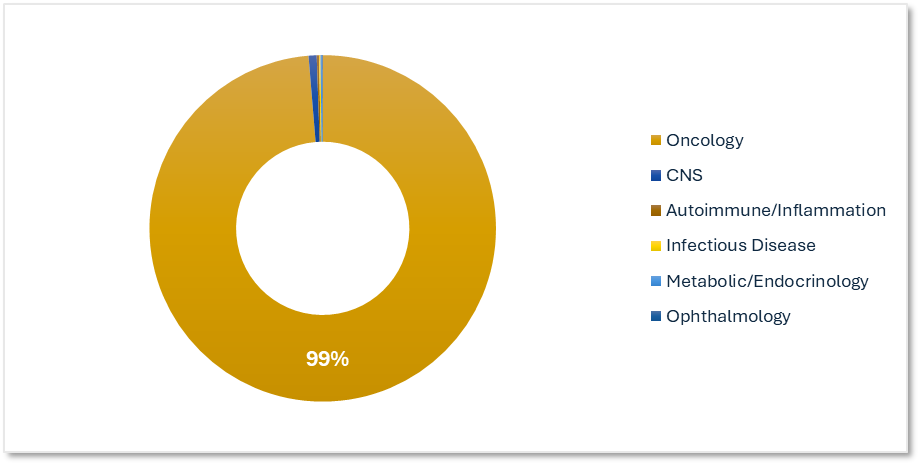
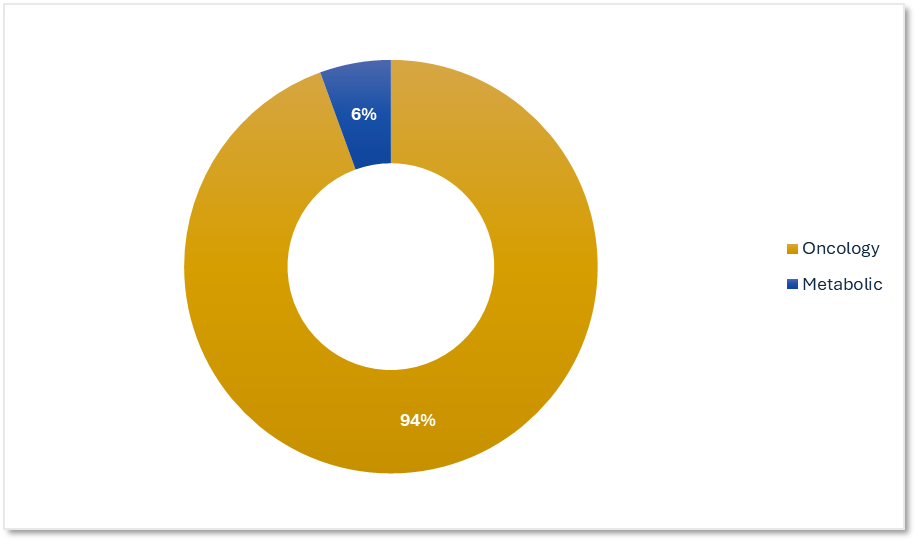
ADC Therapeutic Specialization from an Oncology-focused Clinical Research Organization
Our ADC trials are focused on oncology indications with complex dosing and safety profiles. We help sponsors optimize therapeutic targeting.
Precision for Medicine's ADC Trials by Therapeutic Area
 Citeline Trialtrove® – 07OCT2025
Citeline Trialtrove® – 07OCT2025
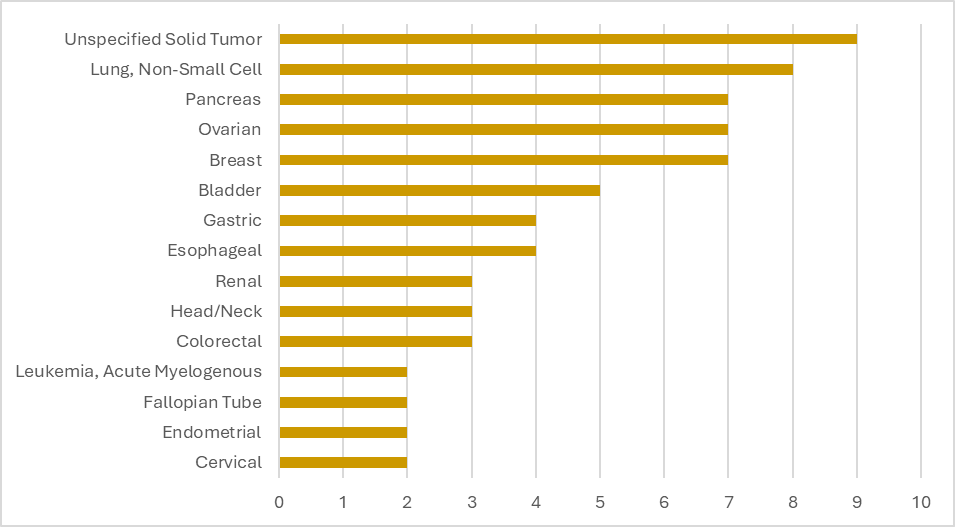
Target Patient Populations: Precision's ADC Indication Expertise
Our portfolio includes studies with the following participant populations, our top indications are NSCLC, Pancreas, Ovarian, and Breast Cancer. With our broad experience, Precision study teams can help sponsors navigate indication-specific challenges.
Precision for Medicine's ADC Trials by Top Indications
 Citeline Trialtrove® – 07OCT2025
Citeline Trialtrove® – 07OCT2025

Partner with Precision for Your Upcoming ADC Clinical Trial
ADC trials require specialized planning and execution, particularly when managing complex dosing schedules and safety oversight. Precision for Medicine works as a partner with our sponsors to operationalize these studies efficiently. From our Precision Site Network (PSN), supporting with feasibility & site selection, to our integrated data management model providing fast data review, our teams bring experience and solution focused study management strategies helping ensure ADC trials are delivered with consistency and clarity across global geographies.
When your ADC program demands both speed and scientific rigor,
Precision for Medicine delivers the expertise to get it right the first time.
-
Explore

Oncology CRO Services
Tomorrow's targeted therapies require a shift away from yesterday's processes. Precision's specialized oncology CRO has integrated and aligned capabilities to efficiently navigate and execute complex clinical trials.Oncology CRO Services
Tomorrow's targeted therapies require a shift away from yesterday's processes. Precision's specialized oncology CRO has integrated and aligned capabilities to efficiently navigate and execute complex clinical trials. -
Explore

Fast Study Startup
Precision's approach to Study Start Up combines technological innovation, regulatory insight, and global expertise to optimize every phase of trial initiation, ensuring your study begins with the momentum needed to succeed.Fast Study Startup
Precision's approach to Study Start Up combines technological innovation, regulatory insight, and global expertise to optimize every phase of trial initiation, ensuring your study begins with the momentum needed to succeed. -
Explore

Speak with an Expert
Ready to meet Precision specialists? Tell us about your program and we'll get back to you right away.
Speak with an Expert
Ready to meet Precision specialists? Tell us about your program and we'll get back to you right away.
References
- Flynn P, Suryaprakash S, Grossman D, Panier V, Wu J. The antibody–drug conjugate landscape. Nat Rev Drug Discov. 2024;23(8):577-578. doi:10.1038/d41573-024-00064-w
- Mullard A. Dual-payload ADCs move into first oncology clinical trials. Nat Rev Drug Discov. 2025;24:573-576. doi:10.1038/d41573-025-00121-y